“Whole-Population” Risk-Adjustment Study Featured in BMC Health Services Research
March 2017 -- As the focus of healthcare transformation shifts from fee-for-service to value-based payments, the need for all-payer – “whole-population” – analyses of system and provider performance has become essential. Fundamental to a value-based payment strategy that supports proactive population health management and system sustainability is the need to adjust for various risk profiles across diverse patient populations. Without accounting for such wide variation and disparity in patient populations (e.g., across commercial, Medicare, and Medicaid payers), the task of reliably measuring, monitoring, and improving the quality of care for a defined population becomes challenging.
In a newly released study, “Risk-Adjustment Methods for All-Payer Comparative Performance Reporting in Vermont,” available free of charge at BioMed Central (BMC) Health Services Research, an international open-access, peer-reviewed journal highlighting innovations in health services research, researchers from Onpoint Health Data and the Vermont Blueprint for Health worked together to evaluate risk-adjustment approaches for the “whole population” to make ongoing research more effective. Applying different levels of risk adjustment to patient-centered medical home (PCMH) populations in Vermont – from a basic model that adjusted only for age and gender to a more comprehensive model that adjusted for demographics, major payer types, and health status information – the study’s results indicate that the more comprehensive risk-adjustment model is more effective for comparing cost, quality, and utilization measures across multi-payer patient populations.
Vermont’s PCMH practices vary significantly in both their adult and pediatric patient populations. Across the entire PCMH program’s adult population, for example:
- The average age of adults varies from 40 years old to 68 years old
- The percent of the population covered by Medicaid ranges from 1% to 48%
- The percent of the population experiencing significant chronic conditions varies from 2% to 36%
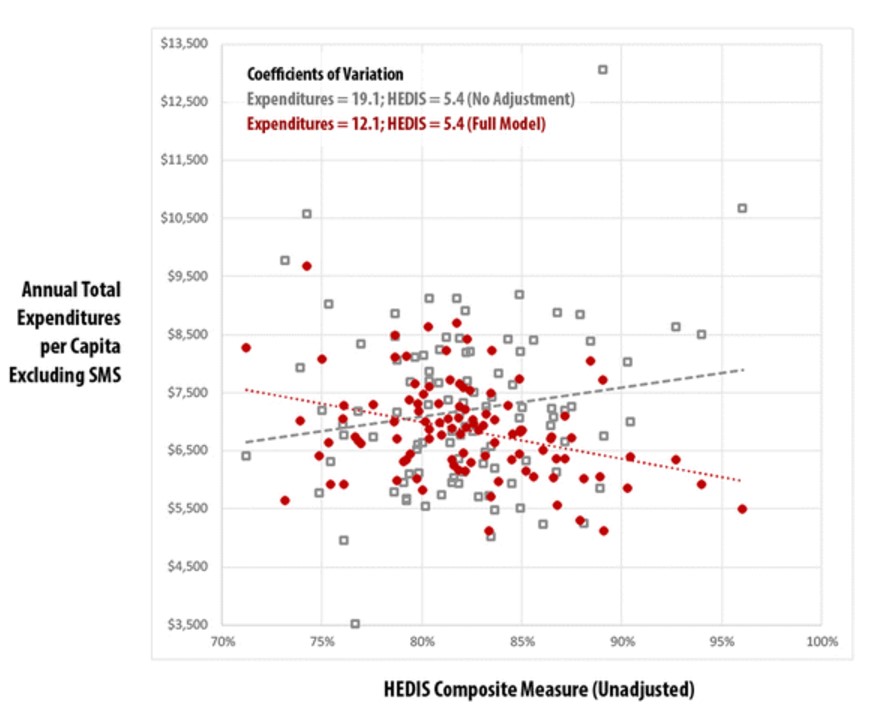
Compared to a model that does not employ risk adjustment, the more robust risk-adjustment model developed in this study greatly reduces the coefficient of variation between practices (i.e., the amount of variability relative to the mean) from 18.5 to 11.7. Relationships among risk-adjusted, practice-level total expenditures and a composite Healthcare Effectiveness Data and Information Set (HEDIS) quality measure are also examined for the adult and pediatric PCMH populations.
The study reveals several important findings related to risk adjustment, measures standardization, and comparability across practices. The analysis concludes that future evaluations “will be important for practices, many of which do not distinguish their patients by payer type and for the implementation of incentive-based or alternative payment systems that depend on ‘whole-population’ outcomes.”
“The analysis demonstrates that, in the absence of any ‘gold standard’ of risk adjustment, it is indeed possible to combine multi-payer populations into a single whole-population measurement system using a more comprehensive risk-adjustment model,” notes Karl Finison, Director of Analytic Development at Onpoint and lead researcher for the study.