Evaluations of Advanced Primary Care Programs Provide Mixed Results
The U.S. Centers for Medicare & Medicaid Services (CMS) recently announced first-year findings from two of its Innovation Center’s programs: the Comprehensive Primary Care (CPC) initiative and the Multi-payer Primary Care Practice (MAPCP) demonstration. These projects are part of CMS’s broader efforts to improve the delivery of care, the health of the overall population, and the cost of healthcare across the country by promoting care coordination and management.
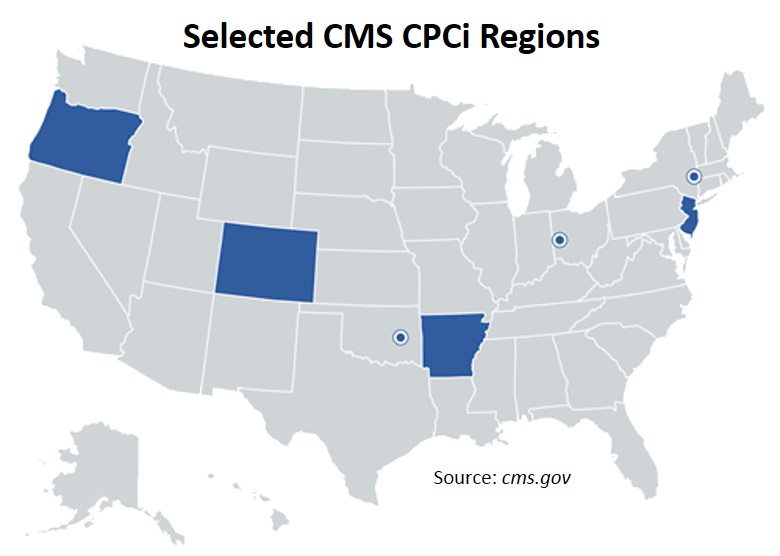
The CPC initiative is a multi-payer partnership between Medicare, Medicaid, and private payers and primary care practices. There are currently a total of seven CPC participants operating in four states (Arkansas, Colorado, New Jersey, and Oregon) and three regions (New York’s Hudson Valley region, Ohio-Kentucky’s Cincinnati-Dayton region, and Oklahoma’s Greater Tulsa region). As a whole, the initiative comprises 492 practice sites with 2,158 participating providers that serve approximately 2.5 million patients.
 Although CMS’s first annual CPC report cautions that “practices vary considerably in their progress on implementing the components of CPC” — with 90% of the CPC practice sites having met first-year practice transformation requirements — findings to date suggest that, overall, the initiative has seen the greatest transformation in hospital readmission rates (2% decrease) and emergency department visits (3% decrease), while generating the bulk of its total savings from patients in the highest-risk quartile.
Although CMS’s first annual CPC report cautions that “practices vary considerably in their progress on implementing the components of CPC” — with 90% of the CPC practice sites having met first-year practice transformation requirements — findings to date suggest that, overall, the initiative has seen the greatest transformation in hospital readmission rates (2% decrease) and emergency department visits (3% decrease), while generating the bulk of its total savings from patients in the highest-risk quartile.
According to Dr. Patrick Conway, Deputy Administrator for Innovation and Quality and CMS Chief Medical Officer, the CPC evaluation demonstrates that the initiative has “generated nearly enough savings in Medicare healthcare expenditures to offset care management fees paid by CMS.” Nonetheless, he advises researchers and stakeholders alike that additional time, resources, and research are needed in order to view a clearer picture of the total effect the CPC initiative is having on its primary care practice sites.
The MAPCP demonstration is also a multi-payer collaboration between Medicare, Medicaid, and private payers and primary care practices. However, while the CPC initiative’s service delivery and payment models have been defined by the Innovation Center at CMS, the MAPCP demonstration’s models have been defined individually by the states participating in the program. Under the MAPCP demonstration, each state has the leeway to design its own approach to multi-payer participation. This freedom, along with a number of other factors (e.g., the specific details of the service delivery and payment models, the size of the programs, and the enrollment processes of the practices involved) help to differentiate the two multi-payer, advanced primary care programs.
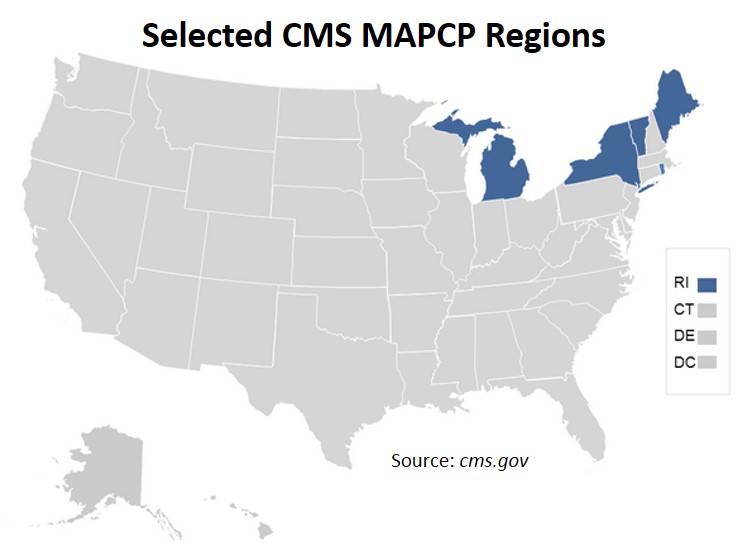 While eight states were initially selected for the MAPCP demonstration (Maine, Michigan, Minnesota, New York, North Carolina, Pennsylvania. Rhode Island, and Vermont), only five have accepted to continue participation in the demonstration through 2016, including Maine, Michigan, New York, Rhode Island, and Vermont. At the end of the demonstration's first year of operation, there were more than 700 participating practice sites with 3,800 providers serving approximately 2.6 million patients.
While eight states were initially selected for the MAPCP demonstration (Maine, Michigan, Minnesota, New York, North Carolina, Pennsylvania. Rhode Island, and Vermont), only five have accepted to continue participation in the demonstration through 2016, including Maine, Michigan, New York, Rhode Island, and Vermont. At the end of the demonstration's first year of operation, there were more than 700 participating practice sites with 3,800 providers serving approximately 2.6 million patients.
While MAPCP programs in two states, Vermont and Michigan, have noted a reduction in the growth of Medicare spending, there so far is little evidence to suggest the program’s overall contribution in improving cost, utilization, or quality of care among the other MAPCP programs. However, the first annual MAPCP report posits that limited evidence of the demonstration’s beneficial outcomes might simply be due to the challenges some participating states have experienced in collecting and using the data derived from their programs.
Despite CMS’s as-yet underwhelming evaluation of its MAPCP demonstration, a study by the Patient-Centered Primary Care Collaborative (PCPCC) with the Milbank Memorial Fund, published in the same general timeframe as CMS released its first annual reports, indicates that the patient-centered medical home (PCMH) model — like the ones built by participating states under the MAPCP demonstration — is actually tied to a number of “impressive and growing trends.”
The study, “The Patient-Centered Medical Home’s Impact on Cost and Quality,” reviewed 28 PCMH evaluation publications, including peer-reviewed literature, state PCMH program evaluations, and industry reports published between September 2013 and November 2014. It reports that the PCMH model has been found to reduce healthcare costs and unnecessary utilization of services, improve population health and preventive services, increase access to primary care, and create satisfaction among patients and clinicians.  Of the 28 PCMH evaluation publications:
Of the 28 PCMH evaluation publications:
- 86% found the PCMH model to reduce unnecessary utilization of services
- 39% found the PCMH model to reduce population health and preventive services
- 36% found the PCMH model to improve access to primary care
- 29% found the PCMH model to create satisfaction among patients and clinicians
Conclusions from the PCPCC review and CMS evaluation suggest that sustained streams of funding for advanced primary care — and, specifically, the PCMH model — can play a valuable role in giving participating practices enough time and resources both to “deepen and refine their methods of delivering advanced primary care” and to sufficiently collect and use the data derived from their programs. By doing so, future evaluations may be better able to judge the effectiveness of the programs in reaching complete multi-payer, primary care delivery transformation.
Explore More
- Indiana Health Prices Chatbot Recognized Nationally with NAHDO 2026 Innovation in Data Dissemination Award
- Staff Spotlight: Kate Davis, MBA, PMP - Client Services Manager
- New Onpoint Issue Brief: Calculating FFS Equivalents for Capitated Services
- Staff Spotlight: Jesse Drummond, PhD - Director of Data Analytics